Why LESS Sensitive Tests Might Be Better
Based on minutephysics's video on YouTube. If you like this content, support the original creators by watching, liking and subscribing to their content.
PCR’s high sensitivity is ideal for diagnosis but can be counterproductive for community screening because it can detect non-infectious viral fragments.
Briefing
More sensitive COVID tests aren’t automatically better for stopping outbreaks. For community screening, slightly less sensitive but much faster and cheaper tests can identify more truly infectious people sooner—so they can suppress transmission more effectively per dollar.
The argument starts with the tradeoffs of the gold-standard nasal swab PCR test. PCR is highly sensitive, meaning it can detect tiny amounts of viral material, which is ideal for diagnosing an individual case. But community screening runs into three practical problems. PCR is expensive, so many places end up testing mainly symptomatic people or those recently exposed—missing a large share of contagious individuals who never develop symptoms. PCR is also slow, with results often taking a couple of days. Since infectiousness typically peaks and then declines, delayed results can miss the period when a person is most likely to spread the virus.
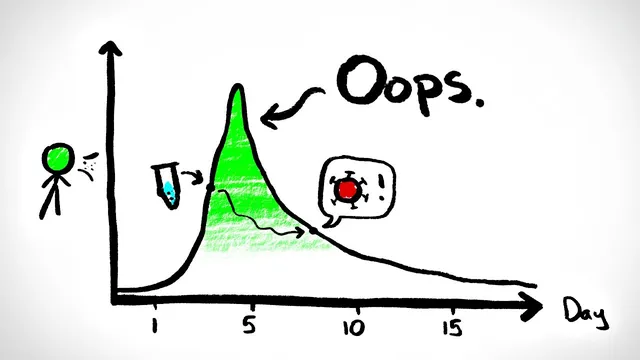
There’s also a subtler downside to PCR’s extreme sensitivity. PCR can remain positive after a person is no longer infectious, because it detects viral fragments rather than viable virus. That means PCR can trigger quarantine and contact tracing for people who pose little or no transmission risk. The goal of screening isn’t just to label every infection; it’s to catch people during the window when they can still infect others.
A less sensitive test changes the balance. If a rapid test is only slightly less sensitive than PCR, it may still catch most highly infectious people near the peak, while missing people who are already past their infectious period—arguably a feature, not a bug, for outbreak control. The key is frequency: a test that’s used far more often can outperform infrequent PCR testing. Even if each individual test misses some infections, the higher testing cadence can increase the overall chance of detecting people while they are still contagious.
This leads to a policy-style conclusion: widespread, frequent rapid testing can deliver more “testing bang for the buck” than relying on slower PCR, provided the rapid tests are much cheaper and fast enough, while remaining only modestly less sensitive. The transcript cites public health analyses comparing how much additional testing different countries needed in fall 2020 to suppress COVID—figures used to support the idea that test cost and implementation constraints can determine whether screening is sufficient.
The caveats are important. Rapid tests are not perfect, so negative results can’t be treated as a guarantee. As long as COVID is circulating, masking and distancing still matter. For people with likely exposure, health guidance discussed here includes quarantining for 14 days even after a negative rapid test, with negative rapid results verified by PCR. The benefits of switching to less sensitive tests also have a limit: if sensitivity drops too far, the cost of missed infections outweighs the gains from more frequent testing.
Finally, vaccines don’t erase the need for testing. Vaccination helps reduce risk, but testing likely remains a major tool for suppression—at least until another set of conditions changes the calculus.
Cornell Notes
Community outbreak screening faces a mismatch between what PCR is optimized for and what public health needs. PCR’s very high sensitivity and accuracy are valuable for diagnosis, but they come with high cost and delays, and they can stay positive after infectiousness has ended. Slightly less sensitive rapid tests can still catch many highly infectious people while being used more frequently and quickly, which increases the chance of detecting contagious individuals during their peak. The net effect can be more infections caught per dollar and faster interruption of transmission. That advantage holds only if rapid tests aren’t too insensitive and if negative results don’t replace core precautions or exposure quarantine guidance.
Why can PCR’s extreme sensitivity be a downside for community screening?
How do cost and turnaround time change the effectiveness of PCR for suppressing outbreaks?
What’s the core logic behind using a slightly less sensitive rapid test more often?
What conditions must hold for rapid testing to outperform PCR in community suppression?
Why can’t negative rapid test results be treated as a full safety guarantee?
Do vaccines make the testing tradeoff irrelevant?
Review Questions
- In what ways can PCR’s high sensitivity increase unnecessary quarantine during community screening?
- Explain how testing frequency can compensate for lower per-test sensitivity, and why this has a practical limit.
- List at least three reasons PCR may underperform rapid testing for outbreak suppression, and connect each reason to transmission timing or program coverage.
Key Points
- 1
PCR’s high sensitivity is ideal for diagnosis but can be counterproductive for community screening because it can detect non-infectious viral fragments.
- 2
PCR testing programs often test too few people due to cost, missing asymptomatic contagious individuals.
- 3
PCR turnaround delays can cause interventions to miss the peak infectiousness window.
- 4
Slightly less sensitive rapid tests can outperform PCR for suppression when they are used more frequently and quickly.
- 5
Rapid testing benefits depend on maintaining relatively high sensitivity; if sensitivity is too low, missed infections outweigh coverage gains.
- 6
Negative rapid tests should not replace precautions, and exposure cases may still require quarantine and PCR verification.
- 7
Vaccines help but do not eliminate the need for testing in suppressing COVID.